Treatment-Resistant Depression: Advanced Therapies, Clinical Challenges, and Care
You followed every instruction. You took the medication. You went to therapy. You allowed time to pass—weeks, and sometimes months—but the depression persisted.
If that sounds familiar, you are not alone. Roughly one in three people treated for major depressive disorder does not experience adequate relief from standard antidepressants. When two or more properly dosed, adequately timed medication trials fail to produce results, what a person is facing has a specific clinical name: treatment-resistant depression, or TRD.
This is not a personal flaw. It is not a failure of willpower. It is a complex neurobiological condition that requires a different level of care, and in recent years, the treatment landscape has shifted in ways that offer real, documented hope. This blog breaks down what treatment-resistant depression actually is, why it develops, and what advanced interventions are now changing outcomes for people who had started to believe nothing would work.
Table of Contents

Resistant Depression and Persistent Symptoms in Mental Health Care
Resistant depression rarely arrives with a clear announcement. Most people who end up with this diagnosis spend a long stretch of time doing everything right, filling prescriptions, attending appointments, trying one medication after another, and still find themselves back in the same dark place.
The symptoms that define resistant depression are not unique, but their stubbornness is. Common persistent symptoms include:
- Persistent low mood that does not lift even during positive life events
- Cognitive fog with difficulty concentrating, making decisions, or following conversations
- Disrupted sleep patterns, whether insomnia or hypersomnia
- Physical fatigue that rest does not resolve
- Loss of motivation or pleasure in activities that once felt meaningful
- Social withdrawal that compounds over time
What clinicians track with rating tools like the Hamilton Depression Rating Scale or the Patient Health Questionnaire is not just symptom presence, but symptom persistence, how long these experiences endure, how much they interfere with daily life, and whether treatment is producing measurable change. When the answers consistently point to “still struggling,” resistant depression becomes the working diagnosis, and the treatment approach needs to evolve accordingly.

Therapy-Resistant Depression and Limitations of Standard Interventions
Standard care for depression is effective for the majority of patients. Antidepressants such as SSRIs, SNRIs, and evidence-based psychotherapy like cognitive behavioral therapy (CBT) work well enough that they remain the appropriate first and second lines of treatment. But for a significant subset of people, these tools hit a wall, and that wall is therapy-resistant depression.
The reasons standard interventions fall short are more varied than most people realize. Common contributing factors include:
- Undiagnosed medical conditions such as thyroid dysfunction, sleep apnea, or autoimmune disorders that mimic or worsen depression
- Undetected bipolar disorder, where antidepressants alone are not the appropriate treatment
- Comorbid anxiety, which often needs separate, targeted management
- Chronic pain conditions that maintain neurobiological stress even when mood-focused treatment is in place
- Substance abuse that interferes with medication metabolism and neurological stability
- Hormonal imbalances, particularly in perimenopause or postpartum periods
In therapy-resistant depression, clinicians are advised to revisit all of these factors before assuming the depression is not treatable.

TRD and Complex Mood Disorder Management
TRD depression is the clinical shorthand, but behind those three letters is a condition that touches virtually every aspect of a person’s functioning. It sits at the intersection of genetics, neuroscience, lived experience, and health system limitations, and managing it requires a level of complexity that goes well beyond writing a new prescription.
Clinicians managing TRD typically work through several strategic layers:
Augmentation strategies involve adding a second agent to an existing antidepressant, rather than replacing it entirely. Common augmentation options include:
- Lithium, which has decades of evidence supporting its role in treatment-resistant cases
- Atypical antipsychotics such as aripiprazole, quetiapine, or olanzapine
- Thyroid hormone (T3) supplementation, particularly in cases with borderline thyroid function
- Buspirone for anxiety-driven mood disruption
Switching strategies involves replacing the current antidepressant with one from a different pharmacological class, moving from an SSRI to an SNRI, a tricyclic, or an MAOI, for example.
Combination therapy uses two antidepressants simultaneously, chosen for complementary rather than overlapping mechanisms.
Beyond treatment-resistant depression medication, biomarker research is beginning to offer new ways of approaching TRD before the trial-and-error process begins. Elevated C-reactive protein, disrupted cortisol rhythms, and glutamate signaling abnormalities are all being studied as potential biological predictors of treatment resistance. As precision psychiatry matures, the goal is to match the right intervention to the right neurobiological profile from the start.

Refractory Depression and Ongoing Functional Impairment
The term “refractory depression” is used when depression has resisted not just first-line treatment but multiple rounds of augmentation and optimization as well. It describes a condition that has proven genuinely intractable, one where even experienced clinicians reach for their most advanced tools.
What makes refractory depression particularly difficult to live with is the breadth of its functional reach. It does not stay confined to mood. Its impact spreads into the following:
- Cognitive performance: memory difficulties, slowed processing speed, and impaired executive function that affect work and everyday tasks
- Occupational functioning: absenteeism, reduced productivity, difficulty maintaining employment
- Parenting and caregiving: the energy required for others becomes nearly impossible to sustain.
- Physical health: disrupted sleep, appetite changes, and reduced activity compound metabolic and cardiovascular risk
- Crisis vulnerability: people with refractory depression have a significantly elevated risk of hospitalization, self-harm, and suicidal ideation compared to those who respond to standard treatment.
This is why identifying refractory depression early and getting the right treatment without delay is both a clinical and a moral priority.

Medication-Resistant Depression and Antidepressant Response Challenges
Medication-resistant depression forces a reckoning with one of psychiatry’s oldest assumptions: if you keep trying antidepressants, one will eventually work. Several factors shape antidepressant response in medication-resistant depression:
- Pharmacogenomics: genetic variations in enzymes like CYP2D6 and CYP2C19 affect how quickly the body metabolizes certain antidepressants. Rapid metabolizers clear drugs before therapeutic levels build; poor metabolizers accumulate them to potentially toxic concentrations at standard doses.
- Episode duration and severity: longer and more severe depressive episodes are independently associated with lower response rates, suggesting that neurobiological changes accumulate over time in ways that affect medication efficacy.
- Episode recurrence: each successive depressive episode that goes inadequately treated may sensitize the brain in ways that reduce response to subsequent pharmacological intervention.
- Inflammatory burden: elevated pro-inflammatory cytokines interfere with serotonin synthesis, reduce neuroplasticity, and disrupt dopamine reward circuits in ways that antidepressants targeting monoamines alone cannot address.
Pharmacogenomic testing is now clinically available and can meaningfully reduce the trial-and-error dimension of managing medication-resistant depression. While it does not guarantee outcomes, knowing a patient’s metabolic profile helps clinicians avoid predictably ineffective or poorly tolerated agents, and that alone can save months of unnecessary suffering.


Understanding the Neurobiological Mechanisms Behind Drug-Resistant Depression
Drug-resistant depression helps to understand why standard antidepressants work at all and why that mechanism eventually stops being enough for some people.
Most conventional antidepressants target the monoamine system, increasing the availability of serotonin, norepinephrine, or dopamine in the synaptic cleft. This approach works for many. But in drug-resistant depression, the problem is not primarily a monoamine deficit. The neuroscience points elsewhere:
- Glutamate dysregulation: NMDA receptors in the glutamatergic system play a central role in synaptic plasticity, learning, and emotional regulation. When these receptors malfunction, the downstream effects on mood and cognition are severe and largely unresponsive to serotonergic agents.
- Reduced neuroplasticity: chronic depression physically reduces the density of synaptic connections in prefrontal regions. Without adequate neuroplasticity, the brain cannot reorganize in ways that support recovery.
- Prefrontal-limbic disconnection: disrupted communication between the prefrontal cortex (which governs rational regulation of emotion) and the amygdala and other limbic structures keeps the nervous system locked in a threat-responsive, dysregulated state.
- Neuroinflammation: elevated inflammatory cytokines appear in a substantial subset of people with drug resistant depression, interfering with neurotransmitter production and blunting the neural reward response.
These neurobiological realities explain why some of the most promising interventions for drug-resistant depression, such as ketamine, esketamine, and TMS, target glutamate signaling and neuroplasticity directly, rather than monoamines.
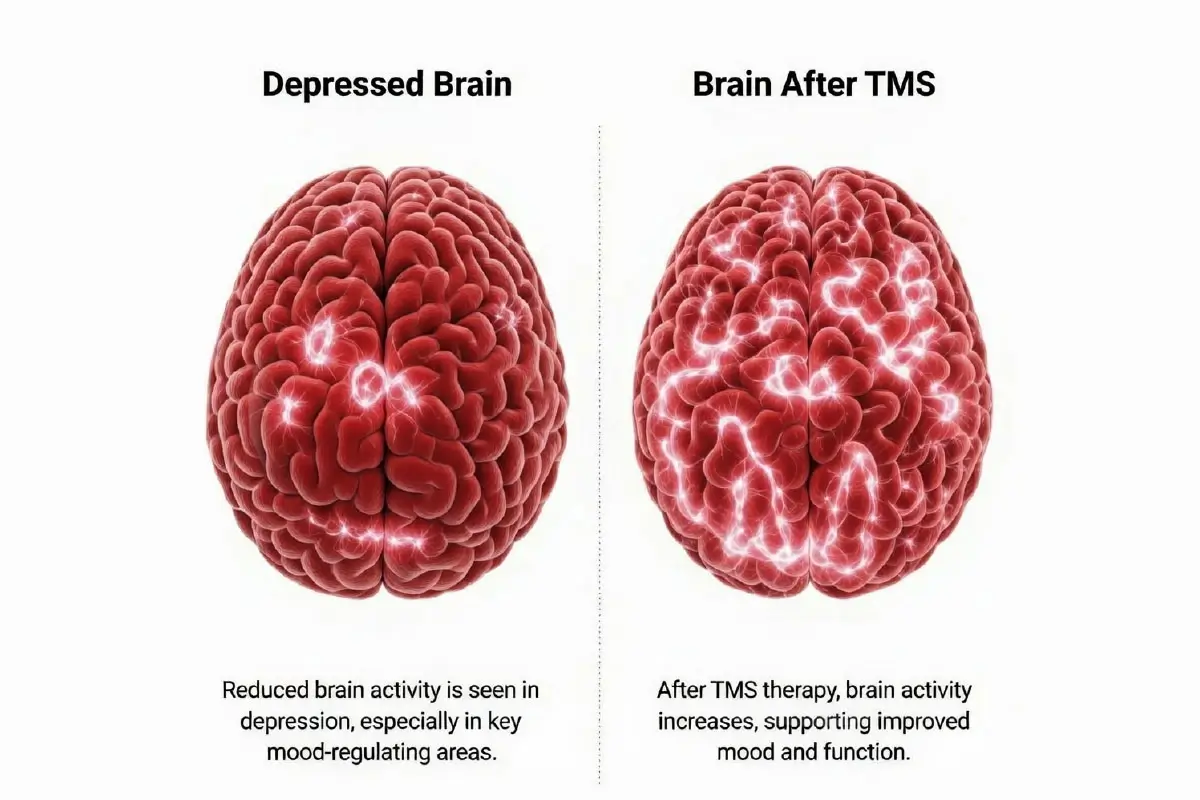
TMS Therapy for Treatment Resistant Depression
Transcranial Magnetic Stimulation, commonly known as TMS Therapy, delivers focused magnetic pulses to the left dorsolateral prefrontal cortex, a region consistently underactive in depression. By stimulating neuronal firing in this area, TMS promotes synaptic strengthening and restores more normal communication patterns between mood-regulating brain networks.
What TMS treatment looks like:
- Administered five days per week over four to six weeks
- Each session lasts 20 to 40 minutes
- No anesthesia, no sedation, no recovery period
- Patients can drive themselves and return to work the same day
What the evidence shows:
- Response rates of 50 to 60 percent among people with depression who are treatment resistant and have failed multiple antidepressants
- Remission rates in the range of 30 to 35 percent
- Newer theta burst stimulation (TBS) protocols compress treatment into as little as three minutes per session with comparable outcomes.
For individuals who have lost confidence that anything will help, TMS offers something different: a non-drug mechanism, a low side-effect profile, and an evidence base built specifically on patients who had already failed standard care. It does not require the body to metabolize a drug, it does not interact with other medications, and it does not carry the systemic risks associated with many augmentation strategies.

Esketamine Therapy for Treatment-Resistant Depression
Esketamine therapy marked a turning point in psychiatric medicine when the FDA approved it in 2019 under the brand name Spravato, the first genuinely new mechanism of action for depression approved in decades. Rather than targeting serotonin, esketamine works on NMDA glutamate receptors, directly addressing one of the core neurobiological drivers of depression treatment resistance.
How esketamine therapy works in practice:
- Self-administered as a nasal spray under direct clinical supervision in a certified healthcare setting such as Mid Cities Psychiatry
- Followed by a mandatory two-hour monitoring period due to potential dissociative effects and blood pressure changes
- Typical schedule: twice weekly for the first four weeks, then weekly, then biweekly as maintenance
- Always used in combination with an oral antidepressant for sustained effect
Why it matters for treatment-resistant depression:
- Clinical trials showed meaningful remission rates within the first four weeks. A timeline that stands in stark contrast to the four to eight weeks typically needed before conventional antidepressants produce any detectable effect.
- For individuals in acute distress or at elevated suicide risk, the speed of esketamine’s action is clinically significant, not just a convenience.
- Works through a mechanism entirely distinct from prior failed medications, meaning previous non-response does not predict esketamine non-response.

Ketamine Infusion Therapy for Treatment-Resistant Depression
Ketamine therapy delivered intravenously has been used off-label in specialized psychiatric and anesthesiology settings for over twenty years. It remains one of the fastest-acting interventions available for medication-resistant depression, with antidepressant effects that can appear within hours of a single infusion.
The standard ketamine infusion protocol:
- A series of six infusions administered over two to three weeks
- Each infusion lasts approximately 40 minutes in a monitored clinical environment.
- Booster infusions used to sustain remission following the initial series
How ketamine works at the neurobiological level:
Ketamine does more than simply block NMDA receptors. Research has clarified that its antidepressant mechanism involves a rapid downstream effect on synaptogenesis, the formation of new synaptic connections. In brain regions like the medial prefrontal cortex, where chronic depression causes measurable structural losses, ketamine appears to restore synaptic density with unusual speed. This synaptogenic effect may explain why some patients maintain antidepressant benefits for weeks after the drug has cleared their system entirely.
For people with medication-resistant depression, the fact that ketamine works through a mechanism completely separate from conventional antidepressants means prior medication failures do not diminish its relevance. It is also worth noting that ketamine infusion therapy has been specifically studied in populations with active suicidal ideation, where its rapid action has shown genuine promise in reducing acute risk.
Treatment-Resistant Depression FAQs
The major depressive disorder therapies are TMS, esketamine, and ketamine infusions. They are evidence-based treatments that carry a completely different approach than oral antidepressants.
Several treatment-resistant depression causes are usually ignored during standard care. Undiagnosed thyroid dysfunction, chronic inflammation, sleep disorders, and hidden bipolar disorder all interfere with antidepressant response without obvious warning signs. Some other treatment-resistant depression causes are untreated conditions, brain chemical disturbances, and psychosocial factors, all of which contribute to treatment-resistant depression.
Treatment-resistant depression causes are rarely the same across two individuals. One person may carry a genetic variant that prevents antidepressants from reaching therapeutic levels. Hormonal imbalances, PTSD, and comorbid anxiety all shape how depression behaves and resists treatment.
Yes, and this is one of the most important things to understand about advanced major depressive disorder therapies. Ketamine works on the glutamate system, not monoamines, so previous antidepressant failures do not reduce its effectiveness.
A good treatment-resistant depression clinic does not hand you another prescription and send you home. It starts with a detailed assessment and finds the underlying causes of the condition. The clinical team builds an individualized plan that may include TMS, ketamine, esketamine, or structured medication management. The difference a specialized treatment-resistant depression clinic makes is not just the tools available but the depth of attention brought to a condition that has already been underserved.
Treatment-resistant depression medication options include lithium augmentation, atypical antipsychotics, MAOIs, and FDA-approved esketamine, each working through a different mechanism than what likely failed before. A specialized treatment-resistant depression clinic can identify which direction makes the most clinical sense based on your specific history, genetics, and symptom profile.
Standard psychiatric care is built around first- and second-line treatments, which is appropriate for most patients. A treatment-resistant depression clinic is specifically structured for the cases that fall outside that range.
Conclusion for Treatment-Resistant Depression
The landscape of care for treatment-resistant depression has changed meaningfully in recent years, and the right clinical team makes all the difference in navigating it. At Mid Cities Psychiatry, we specialize in treating medication-resistant depression. From TMS therapy and esketamine to ketamine infusions and comprehensive psychiatric medication management, our team brings advanced, evidence-based interventions together under one roof built specifically for people who need more than the standard approach. Recovery from treatment-resistant depression is rarely linear, and it is rarely quick. But it is possible, and you do not have to keep searching for answers alone. If you or someone you love is still struggling despite multiple treatment attempts, reach out to Mid Cities Psychiatry. We are here to help you live a happy and healthy life.
Revision History
Author

Dr. Sacha Cohen
Medical & Clinical Educator
Dr. Sacha Cohen is a healthcare professional and medical content writer with experience in clinical training and academic writing. She specializes in creating research-based, accessible healthcare content. With a foundation in medical education and hands-on clinical practice, she brings depth and clarity to every piece she writes. Passionate about making medical knowledge understandable, she aims to educate and inspire her readers.

Dr. Kazi, Seema
Dr Seema Kazi is a board-certified psychiatrist and a proficient Medical Director of Mid Cities Psychiatry at Euless, Texas.
Fact Checker

Dr. Seema Kazi
Founder & Medical Director
Dr. Seema Kazi is the compassionate force behind Mid Cities Psychiatry, where her vision has shaped a practice rooted in empathy, excellence, and patient-centered care. As a triple board-certified psychiatrist in Psychiatry, Geriatric Psychiatry, and Internal Medicine, Dr. Kazi brings over 20 years of clinical experience to her leadership role.